
Last updated on December 10th, 2024 at 05:07 am

Take Home Points
- EMS Structure: Emergency Medical Services (EMS) integrate dispatch, EMTs/paramedics, and EM physicians for pre-hospital patient care and transport, with variations in service models (public, private, or fire-integrated).
- EMS Certification Levels: Nationally, there are four EMS provider levels—Emergency Medical Responder (EMR), Emergency Medical Technician (EMT), Advanced EMT (AEMT), and Paramedic—each with progressively advanced training and scope of practice.
- Key Roles of EMTs: EMTs are the baseline for independent ambulance operation, responsible for assessing, stabilizing, and transporting patients, with training in triage and basic interventions like oxygen, nitroglycerin, and CPR.
- Paramedic Expertise: Paramedics offer advanced care, including cardiac monitoring, rapid sequence intubation (RSI), and critical interventions, often addressing emergencies comparable to initial emergency department care.
- Scope Variation: EMS protocols and capabilities differ by state and agency, influencing medication administration and advanced procedures such as RSI or cricothyrotomy.
All physicians need to know how to interact with the EMS service and understand the basics of care and different levels of service. EM physicians must have a special understanding of the role they play with the EMS service and how they can best interact and occasionally direct their EMS colleagues.
Emergency Medical Services (EMS) is a comprehensive system involving the identification, response, treatment, and transport of patients requiring medical evaluation and care. A well-run system involves the integration of emergency dispatch, EMTs/paramedics, and EM physicians in the care of patients.
Generally speaking there are three main types of EMS agencies that provide ambulance transport to hospitals and other locations.
- Many larger cities run combined Fire and Emergency Medical Services (FEMS) in these agencies most providers are dual certified as Firefighters (FF) and as Emergency Medical Technicians (EMT) with some providers being both FF and paramedics.
- It is also common to have separate city or county run agencies where the fire and EMS services are separate and all of the providers are EMTs with some being paramedics.
- There are also private EMS agencies, these agencies can be contracted with the city/county to provide typical 911 EMS services, but they often work as interfacility EMS transport, staffing for large events or sporting activities, or transport of bed-bound individuals to medical appointments.
Ambulance Provider Levels of Care
Various providers work and operate on ambulances, bringing variety in training and scope of practice to the pre-hospital setting. While each state has various regulations and licensing responsibilities the National Registry of Emergency Medical Technicians (NREMT) provides a national framework and testing scheme for providers. Historically, each state had separate testing to license providers leading to vastly different training and scope of practice between different states. The NREMT consolidated testing and provides for a unified training regimen making sure all NREMT certified providers meet the same minimum competency. Most states now require that providers pass the NREMT examination and maintain a current certification in order to be licensed by the State EMS Board. 12
The NREMT recognizes four different certification levels:
- Emergency Medical Responder (EMR)
- Emergency Medical Technician (EMT)
- Advanced Emergency Medical Technician (AEMT)
- Paramedic (NRP)
The EMT is the minimum level required to operate independently on an ambulance. Each additional level from Advanced to Paramedic denotes additional experience and scope of practice. The names for these roles have changed slightly over the years and you might hear different terminology when talking to providers. EMT’s for example might refer to themselves as EMT-Basics or just “Basic” as this was the previous NREMT term for the role. This has gone out of style as all pre-hospital providers are highly trained and provide much needed life-saving care to our patients. Similarly paramedics might refer to themselves as Advanced Life Support (ALS) providers as they are capable of providing care in line with the Advanced Cardiac Life Support (ACLS) guidelines.
Emergency Medical Responder (EMR)
The EMR level is the first certification for pre-hospital medical providers. They are equipped to identify life-threatening situations and conditions and provide initial stabilization until a higher level of care arrives. While they can assist in the transport of a patient on an ambulance they should not be the sole provider during transport. In rural areas or those with low call volumes an EMR might be the first provider on scene to care for patients while an ambulance arrives with additional equipment and personnel.
Most fire departments train all their members to at least the EMR level so they can provide initial medical care for patients on scene. Many fire departments are going beyond this and training all their members to the EMT level. Many law enforcement officers will also obtain this training though it is less common than with fire personnel.
EMR training focuses on assessing for immediate life-threats and the initial stabilization of those conditions. Medication administration will vary by location but often includes epinephrine auto-injector use, intranasal naloxone, and oxygen administration. In medical situations they will be able to assess the airway, breathing, and circulation as well as provide interventions such as oxygen, mechanical ventilation with a BVM, and CPR using the Basic Life Support (BLS) algorithm. In trauma situations they will be able to assess for life-threatening bleeding and intervene with direct pressure, wound packing, and tourniquet use.
Emergency Medical Technician (EMT)
The EMT level is the minimum requirement to transport independently on an ambulance and is often the first level providers will obtain in pre-hospital medical care. Unlike the EMR level the EMT level is needed initially before providers can train for the AEMT or Paramedic roles. It forms the basis of pre-hospital scene management, assessment, treatment, and transport decision. EMTs can transport patients in any condition though they will request paramedic assistance if available. Some EMS systems will have very limited access to paramedics and will rely on EMTs to transport patients in critical condition.
EMTs are employed in a variety of situations. They can function on ambulances as the sole provider or be paired with another EMT, AEMT, or paramedic. They will often staff first aid tents and work on bike teams, or foot teams for large event management. In the hospital they will often work as emergency department technicians. Many larger fire departments are working to have all their members trained to the EMT level to allow for an increased level of care but also to allow for increased ambulance staffing.
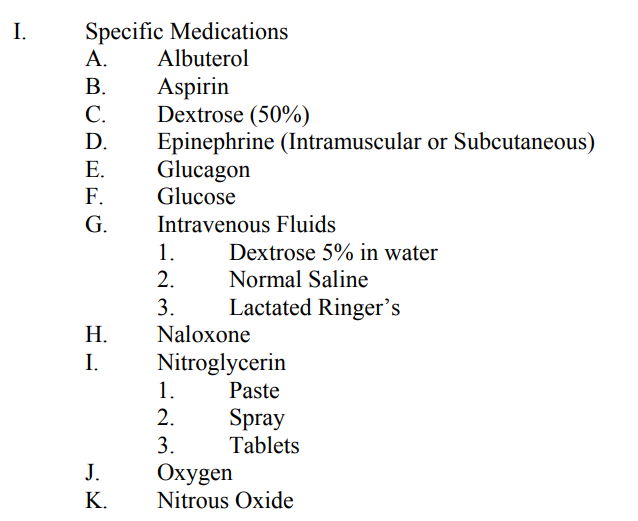
EMT training expands on the EMR scope and includes assessing for underlying disease states and pathology as well as identifying and treating life-threats. Importantly their training focuses on triaging patients to different levels of care and identifying who can be transported at the BLS level and who would need additional resources offered by a paramedic. They will also decide which patients need to be transported emergently verses routine to the hospital. In addition to the skills of an EMR the EMT scope of practice includes additional medications such as albuterol, nitroglycerin, nitrous oxide, aspirin, and epinephrine.
Advanced Emergency Medical Technician (AEMT)
The AEMT operates in a unique space between the level of the EMT and Paramedic roles. Candidates should already have completed EMT training prior to starting their AEMT training. AEMTs often work on ambulances as an ALS adjunct, able to provide more advanced medications and treatment than an EMT. AEMT training locations can be difficult to find as most providers and agencies prefer going straight to the paramedic level after EMT training. Special operations units will sometimes encourage their providers to take this training as it allows for more advanced treatment options without having to go through the longer paramedic training program.
The biggest difference EMT and AEMT is the ability to start and use IV medications. In addition they have a slightly expanded range of medications they can use. Below is a list of medications AEMTs can give in almost every state from the National Highway Traffic Safety Administration (NHTSA) educational course objectives for AEMT training.
The individual state scope of practice for AEMTs varies much more than that of EMTs or paramedics. If you operate in an area with AEMTs knowing their scope of practice will be important when interacting with prehospital providers. Washington D.C. does not license at the AEMT level so those with AEMT training only operate at the EMT level. Virginia does allow for AEMT providers and a list of some expanded medications can be found below. It is important to note that AEMT are not trained to interpret a cardiac monitor and cannot give many of the cardioactive medication that a paramedic can administer. When the AEMT is allowed to give medications such as amiodarone or lidocaine it is only in the cardiac arrest setting.3
| States | Opiates | Benzos | Amiodarone | Lidocaine | Ondansetron | Tylenol/NSAIDs | Antihistamine | Steroids |
|---|---|---|---|---|---|---|---|---|
| Alabama | IN only | x | x | x | x | |||
| Maine | x | x | ||||||
| West Virginia | x | x | x | x | x | x | ||
| North Carolina | x | x | ||||||
| Virginia | x | x | x | x | x | |||
| Kansas | x | x | x | x | x | x | x | x |
| Massachusetts | x | x |
Nationally Registered Paramedic (NRP)
The paramedic is typically the most advanced prehospital provider. They can operate in a variety of situations from the ambulance, advanced first aid, hospital, and many others. The training pathway from EMT to paramedic is typically two years and often grants an associates degree though this is not required. The paramedic has a wide range of medications from cardioactive medications, vasopressors, pain medications, and sedatives. Most of what can be done in the first five minutes in the emergency department can be accomplished by a paramedic on an ambulance. Paramedics are considered Advanced Life Support (ALS) providers and can operate the complete ALS cardiac arrest algorithm.4
The training of paramedics is fairly standardized by the NREMT and the NHTSA but the scope of practice changes by state. Typically the scope of practice is more restrictive than the initial training level of the NREMT. When working on an ambulance most paramedics are partnered with an EMT to assist with treatment and transport. Some agencies staff double paramedic ambulances, though with the current shortage of paramedics this is becoming less common. In the critical care settings paramedics might be partnered with a flight nurse or critical care nurse for advanced medications or treatment options.
There are many changes from the EMT or AEMT level to the paramedic level. These include advanced cardiac monitoring, advanced airway interventions, ALS medications, and an expanded knowledge of anatomy and pathophysiology. Their training includes advanced airway maneuvers include standard and rapid sequence intubation, direct airway foreign body removal, and cricothyrotomy. Respiratory interventions include CPAP, ventilator use, needle and finger thoracostomy. For cardiac interventions they can obtain and interpret EKGs, work through the full ALS pathway for tachyarrhythmias, bradycardia, and cardiac arrest.
While all paramedic training covers these interventions, individual state scope of practice or agency medical directors might restrict some of these skills depending on provider comfort and agency setting. For example, for Washington D.C. Fire and EMS (FEMS), paramedics do not RSI for intubation. This is due in part to short hospital transport times reducing the need for intubation prior to arriving at the ED. In contrast Fairfax County in Virginia, which is a few miles away, allows paramedics to RSI partly due to the longer transport times making transport without a secured airway unsafe. Cricothyrotomy and finger thoracostomy are other skills that are often restricted by individual agency or state scope of practice.
Specialty and Advanced Practice Paramedics
There are a variety of roles for paramedics beyond the traditional 911 ground transportation model. In the emergency department you will have interactions with flight and critical care transport paramedics, EMS agency supervisors, and possibility even community paramedics.5 The NREMT certifies providers at the EMR, EMT, AEMT, and Paramedic level but for those wanting to practice in critical care or flight settings the International Board of Specialty Certification (IBSC) provides additional testing opportunities.6 The IBSC offers a variety of certifications in flight paramedicine, critical care transport, advanced tactical certification, and community paramedicine. While not required for state licensing most critical care and flight transport agencies require certification by the IBSC for their providers. The examinations go beyond basic paramedic knowledge and will cover in depth knowledge such as advanced ventilator management, multiple vasoactive medication infusions, and aerospace medicine.
Supervisors
Many agencies will have paramedics designated as supervisors. While there is no specific certification for these providers they will significant experience with that agencies protocols and local transport destinations. Depending on the agency the might have additional skill sets such as RSI capability, use of ultrasound, or whole blood administration. They will often have a SUV to respond to critical patient situations and will ride into the hospital if needed to assist the paramedics on scene. Specifically in Washington D.C. the EMS supervisors carry whole blood for unstable patients with active bleeding.
Summary
There are three levels of ambulance staffing, the EMT, AEMT, and paramedic provider. EMTs can provide vital sign monitoring, bleeding control, and a limited amount of medications. They can triage various patient presentation and decide on transport priority and if an ALS provider is needed. The AEMT has an expanded scope of medications specifically the ability to start IV lines and administer IV medications. They function between the EMT and paramedic scope of practice and are mostly utilized in rural medicine settings or specialty rescue/tactical settings where a paramedic might not be available. Paramedics have the full scope of ALS training with a variety of medications available and the ability to independently interpret and intervene with a cardiac monitor/defibrillator. Most flight and critical care agencies expect additional certification for their providers in advanced critical care techniques. While all paramedics receive some training in critical care transport additional certification provides much more familiarity with what would be expected for ICU to ICU transport.
As an emergency medicine physician make sure you are familiar with the prehospital providers in your area, including the skills and scope of practice that is available to them. Knowing their skill sets will allow you to effectively communicate with these providers during hospital handoffs but also when they are calling into the hospital with pre-arrival communication or asking for additional orders. The scope of practice changes based on individual state and locality so reach out to your local EMS agency or hospital leadership for what to expect from providers in your area.
Author
Cite this post: Timothy Harmon, MD. “What to Expect when you’re Expecting… a Patient: A guide to EMS Providers for Emergency Physicians”. GW EM Blog. 12/8/2024. Available at: https://gwemblog.com/ems-providers-guide/
Related Posts:
Tuning In: An Intro to the Radio
rMETRIQ Score: Not yet rated/21
References
- “Information for the Public.” National Registry of Emergency Medical Technicians,
www.nremt.org/Document/public-ems. Accessed 2 Dec. 2024. ↩︎ - National Emergency Medical Services Education Standards, Department of Transportation,
National Highway Traffic Safety Administration, 2021. ↩︎ - National EMS Scope of Practice Model 2019, National Highway Traffic Safety Administration,
2019. ↩︎ - “What’s the Difference between an EMT and a Paramedic?” UCLA CPC, 13 Nov. 2023,
www.cpc.mednet.ucla.edu/node/27. ↩︎ - “How to Become a Flight Paramedic.” EMS1, 21 Aug. 2024, www.ems1.com/ems-
education/articles/how-to-become-a-flight-paramedic-op7Ug5IiYrMGwX4S/. ↩︎ - “About the IBSC & the BCCTPC.” IBSC & BCCTPC – About Us,
www.ibscertifications.org/about/about-us#gsc.tab=0. Accessed 2 Dec. 2024. ↩︎