
: A Rapid Overview")
Take Home Points
- ECMO is a temporary life-support system providing oxygenation, CO₂ removal, and/or circulatory support for severe respiratory or cardiac failure unresponsive to conventional treatments.
- The key indications for ECMO boil down to providing a bridge from life threatening but temporary cardiac or respiratory pathology
- The key contraindications for ECMO are advanced age, irreversible multi-organ failure, contraindications to anticoagulation, and conditions with no potential recovery or bridge to intervention (“bridge to nowhere”).
- Numerous complications exist, include bleeding, thrombosis, infections, limb ischemia, and post-ICU syndrome, with unique risks like Harlequin syndrome in VA ECMO due to differential oxygenation.
Introduction
- What is ECMO?
- ExtraCorporeal Membrane Oxygenation
- An advanced temporary life support for patients with respiratory or cardiac failure not responding to standard therapy
- An external circuit that provides oxygenation, carbon dioxide removal, and/or circulatory support
How ECMO Works
- Basic Physiology
- ECMO involves diverting blood from the patient’s circulation, passing it through an artificial membrane lung, and returning it to the body
- A simplified circuit consists of: drainage and reinfusion cannulae, a pump, membrane lung, heat exchanger, oxygen source, blender, and connection tubing
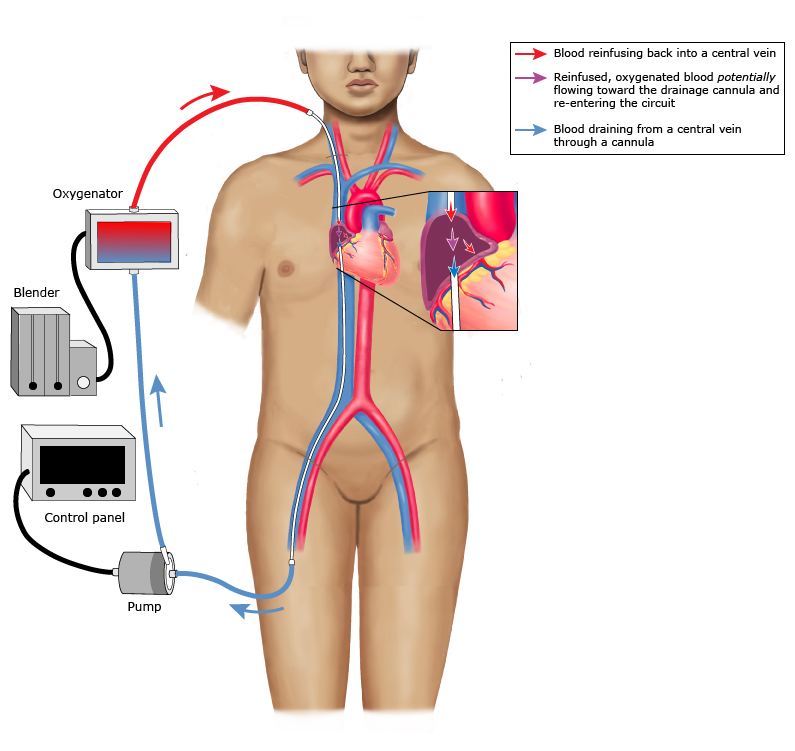
- Venovenous (VV) ECMO1
- A pump generates negative pressure via the “drainage” cannula (typically in the femoral vein or internal jugular [IJ]) and then pumps blood across a membrane lung or oxygenator
- Oxygenated blood is returned to the body via the “return” cannula, typically positioned in a central vein or the right atrium, adding the artificial “lung” in series with the native lung
- Relies on the patient’s heart to circulate the oxygenated blood
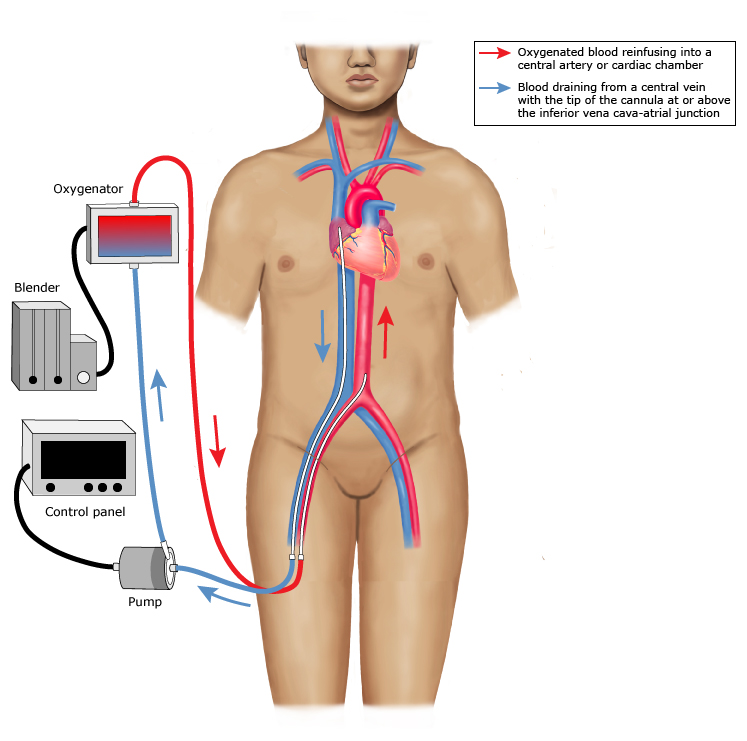
- Venoarterial (VA) ECMO
- Drainage cannula receives blood from the femoral vein and the pump delivers it through the membrane lung/oxygenator, same as VV ECMO
- Oxygenated blood is then pumped back into a central artery (femoral artery or aortic arch)
- Pump also provides continuous circulatory support in place of (or in addition to) the native heart
- Circuit runs in parallel to the native heart/lungs
Indications for ECMO
- Respiratory Indications (VV ECMO)
- Refractory hypoxemia or hypercapnia despite optimal vent settings
- Severe Acute Respiratory Distress Syndrome (ARDS), pulmonary hemorrhage, pulmonary contusion, inhalation injuries (including drowning, smoke, aspiration), status asthmaticus, massive air leak syndromes (e.g. large bronchopleural fistula)
- Bridge to lung transplant
- Cardiac Indications (VA ECMO)
- Left and/or right-sided heart failure
- Cardiac arrest (in which case ECMO is referred to as E-CPR)
- Cardiogenic shock due to myocardial infarction (MI), cardiomyopathy, acute fulminant myocarditis, acute graft failure post-transplant, refractory arrhythmias, right heart failure due to massive pulmonary embolism (PE) or pulmonary hypertension
- Bridge to heart transplant or corrective surgical procedure, Left Ventricular Assist Device (LVAD), etc
- Refractory shock due to other conditions including trauma, anaphylaxis, poisoning, hypothermia
Contraindications to ECMO
- General Contraindications
- Advanced age, typically >75
- Significant comorbid disease i.e. metastatic cancer, advanced cirrhosis, end stage renal disease (ESRD)
- Contraindication to anticoagulation (i.e. intracranial hemorrhage)
- Morbid obesity/habitus that would make cannulation impossible
- Irreversible multi-organ failure
- One of the most important considerations to proceed with ECMO is whether it will provide one of the following:
- A bridge to recovery (is the disease potentially reversible?)
- A bridge to life-saving intervention, such as lung or heart transplant, LVAD, coronary artery stenting or coronary artery bypass graft (CABG), etc.
ECMO is not appropriate for patients in whom these are not achievable (ECMO as a “bridge to nowhere”)
- V-V Specific Contraindications
- Chronic severe pulmonary hypertension
- Prolonged ventilation >7 days with plateau pressures (Pplat) >30 cm and FiO2 >90%
- V-A Specific Contraindications
- Unwitnessed cardiac arrest, prolonged downtime or CPR > 60 minutes prior to commencement of cannulation
- Aortic dissection
- Significant aortic valve incompetence
Complications of ECMO
- Acute Complications
- Hemorrhage (cannula sites, surgical sites, other such as gastrointestinal, intrathoracic, intracranial or retroperitoneal)
- Thrombosis (circuit-related, cannulae-related, arterial or venous thromboembolism)
- Infection (eg, surgical site, systemic), causative organisms often include coagulase-negative Staph, Candida, and Pseudomonas
- Hemolysis
- Thrombocytopenia, including heparin-induced thrombocytopenia
- Vascular perforation during cannulation
- Acute kidney injury is common due to reperfusion injury
- Limb ischemia (common with VA ECMO particularly when using a femoral arterial return cannula which can obstruct flow to the distal ipsilateral leg)
- North-South Syndrome: When the femoral artery is used there is a risk of poor perfusion of the upper extremities and the brain if oxygen is preferentially delivered to the lower extremities and abdominal circulation, especially as the native heart recovers and pumps poorly oxygenated blood from the injured lungs. This phenomenon is also called Harlequin syndrome, dual circulation, or differential hypoxemia.
- Long Term Complications
- Physical, psychological and neurocognitive complications similar to that experienced by other critically ill patients with post-intensive care unit syndrome
E-CPR: What does the evidence say?
- ARREST trial, 20202
- Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST)
- Single center, open-label randomized control trial (RCT)
- Two groups of patients in cardiac arrest with a shockable rhythm: a group that was immediately placed on V-A ECMO vs. a group that received standard ACLS
- Primary outcome was survival to hospital discharge
- The trial was stopped by the Data and Safety Monitoring Board after 30 patients
- 43% in the ECMO group (6 of 15 patients) vs 7% in the standard ACLS group (1 of 15 patients) survived to hospital discharge (risk difference 36%, 3.7-59.2%; 0.986 probability of ECMO superiority)
- INCEPTION trial, 20233
- Early Extracorporeal CPR for Refractory Out-of-Hospital Cardiac Arrest (INCEPTION)
- Multicenter RCT conducted in the Netherlands
- eCPR vs. conventional CPR for refractory cardiac arrest with an initial shockable rhythm
- Primary outcome was favorable neurologic outcome at 30 days
- 20% of the 70 patients who received eCPR had a favorable neurologic outcome as compared to 16% of the patients who received traditional CPR (OR 1.4, CI 0.5 to 3.5; p=0.52).
- Criticisms of this study include longer times from arrest to cannulation (mean 74 minutes), early withdrawal of life-sustaining therapies, and low case volume
The Current State of ECMO and Future of ECMO
In the future, membrane lungs could be paracorporeal (wearable like an LVAD device) for long term use, such as while awaiting transplant. With current technology, a subset of patients may walk, eat, and talk while on ECMO. More and more emergency departments have an ECMO team available 24/7 that can emergently cannulate a patient in cardiac arrest. A few regions offer mobile ECMO units which allow for cannulation in the field. Select patients may live on ECMO for over a year as they receive treatment or as a bridge until possible solid organ transplant.4
Summary
Extracorporeal Membrane Oxygenation (ECMO) is an advanced life support system used for patients suffering from severe respiratory or cardiac failure when conventional treatments are insufficient. ECMO functions by diverting blood from the body, oxygenating it through an artificial membrane lung, and returning it, thus supporting oxygenation and circulation. There are two main types: Venovenous (VV) ECMO, which relies on the patient’s heart for circulation, and Venoarterial (VA) ECMO, which provides both respiratory and circulatory support. Indications for ECMO include refractory hypoxemia, severe acute respiratory distress syndrome, heart failure, and cardiac arrest, among others. However, contraindications exist, such as advanced age and significant comorbidities. Complications can range from acute issues like hemorrhage and thrombosis to long-term psychological effects. Recent trials indicate ECMO’s potential benefits in resuscitation scenarios, and advancements may lead to more innovative, long-term use options in the future.
Author
Cite this post: Jordan Detrick, MD. “Extracorporeal Membrane Oxygenation (ECMO): A Rapid Overview”. GW EM Blog. 12/25/2024. Available at: https://gwemblog.com/ecmo-overview/
Related Posts:
rMETRIQ Score: Not yet rated/21
References
- Abrams D, Agerstrand C, Fried J, Brodie D. Extracorporeal life support in adults in the intensive care unit: Overview. UpToDate. July 19, 2023. Accessed September 24, 2024. https://www.uptodate.com/contents/extracorporeal-life-support-in-adults-in-the-intensive-care-unit-overview?search=ecmo&source=search_result&selectedTitle=1%7E150&usage_type=default&display_rank=1 ↩︎
- Yannopoulos D, Bartos J, Raveendran G, et al. Advanced reperfusion strategies for patients with out-of-hospital cardiac arrest and refractory ventricular fibrillation (ARREST): a phase 2, single centre, open-label, randomised controlled trial. Lancet. 2020;396(10265):1807-1816. doi:10.1016/S0140-6736(20)32338-2 ↩︎
- Suverein MM, Delnoij TSR, Lorusso R, et al. Early Extracorporeal CPR for Refractory Out-of-Hospital Cardiac Arrest. N Engl J Med. 2023;388(4):299-309. doi:10.1056/NEJMoa2204511 ↩︎
- Bartlett, R. ECMO: The Next Ten Years; The Egyptian Journal of Critical Care Med. 2016; vol 4,7-10. doi.org/10.1016/j.ejccm.2016.01.003. ↩︎